Chapter 1: The science and the scan
"Boring, But Necessary"
- Hybrid Imaging System
- Anatomic & Functional Exam
- The Machine
- “Whole Body” vs. “Skull Base to Mid-Thigh”
- Three Sets of Images
Produced
- Glucose Analog
- Malignancy & Glucose Metabolism
- Mechanisms for Increased Intracellular Glucose
- Why 18F-FDG Works
- Whole Body Assessment
- The “You’re Kidding Me!” Effect
- Post-Therapeutic Scar vs. Active Malignancy
- Detecting Malignancy
- Staging Malignancy
- Assess Response to Therapy
- Detecting Recurrence
- Not All Cancer is FDG-Avid
- Normal FDG-Uptake vs. Pathologic Uptake
- Technical Limitations
- Poor Patient Preparation
- Misregistration
- Brown Fat Activation
- SUV Problems
- Fields of View Discrepancy
- PET/CT Artifacts
- Timing of Exam After Therapy
- CT Images
- Non-Attenuation Corrected Images
- Attenuation Corrected Images
- Maximum Intensity Projection (MIP)
- Fusion of Images
- All Images Viewed in 3 Planes
7. Contrast Media: Oral & I.V.
- Who Gets Oral Contrast?
- Who Gets IV Contrast?
- Oral Contrast “Cocktail” Recipe
8. What the Patient Should Expect
- Documenting Height & Weight
- Private Resting Room
- Drinking PO Contrast
- FDG Injection
- Delay Between Injection & Scan
9. Safety Concerns with PET/CT Imaging
- Radiation Exposure to Patient
- Radiation Exposure to Patient’s Contacts
- Patient Contact with Pregnant Women
- Breastfeeding
Chapter 2: PET/CT Problems Which Limit Interpretation
"Something just doesn't seem right here"
- Optimizing Glucose & Insulin Levels
- Fasting Prior to Exam
- Diabetic Patients
- Low Carbohydrate Diet
- Hydration
- Strenuous Exercise
- Voiding Prior to Exam
- Patient Instruction Sheet
- Definition
- Distribution / Appearance
- Don’t Miss the Hidden Nod
- Reporting Language
- Prevention
3. Timing of PET/CT Exam After Therapy
- “Rule of 3”
- Chemotherapy: 1 month
- Surgery: 2 months
- Radiation: 3 months
- Etiology: Hybrid Imaging
- Patient Movement
- Respiratory Motion
- Breathing Techniques
- Bowel Peristalsis
- False Positives
- False Negatives
- Reporting Language
- Beam Hardening
- Diaphragmatic Mismatch
- Linear Hand Motion
- Attenuation Correction
- Differing Fields of View
- Poor Patient Preparation
- FDG Extravasation
- Extensive Brown Fat
- Metformin-Induced Bowel Uptake
- Marked Reactive Marrow Uptake
- Extensive Tumor Uptake in
- Different Types of SUV Measurements
- Factors that Influence SUV Measurements
- What SUV Number Indicates Malignancy?
- What Percent Change in SUV on a Follow Up Exam is Significant?
- How to Compare Exams With Very Different Background Metabolic Activities?
Chapter 3: The Standardized Uptake Value (SUV)
"The good, the bad & the ugly"
1. What is the SUV & Why Used?
- Quantitative vs. Qualitative Assessment
- Unitless Measurement
- Formula
- SUV = ?
- Patient Preparation
- Time Between FDG Injection & Scan
- Partial Volume Effects
- Extravasation
- Patient Weight
- Size & Position of ROI
- Attenuation Correction Artifacts
- Consensus?
- Body Weight
- Lean Body Mass
- Ideal Body Weight
- Body Surface Area
- Maximum vs. Mean
- Average SUV’s by Organ
4. Interpreting the SUV: Threshold Values, “Oncologic Plausibility” & Relative Uptake
- Precise Threshold Values?
- “Oncologic Plausibility”
- Relative Uptake
- Assessing Nodes in Lymphoma Cases
- Assessing Nodes in Non-Lymphoma Cases
- Potential Lesions in Solid Organs
- Pulmonary Nodules
5. What % Change in SUV on a Follow Up Exam is Clinically Significant?
- The Problem
- Current Recommendations
6. How to Compare Sequential Exams With Very Different Background Activities?
- Differing Background Metabolic Activities
- When Qualitative Assessment is Required
- Reporting Language
7. Should We Just Abandon the SUV?
- Pros & Cons
- “Qualitative” Definitions
- Mild
- Moderate
- Intense
- Final Recommendations
Chapter 4: Our Systematic Approach to Reading a PET/CT
"Eat your vegetables"
1. Reading Station & Reading Software
- Reading Station
- Monitor Set-Up
- PET/CT Reading Software
- Hanging Protocol
- Reading in Context (“Oncologic Plausibility”)
- Measure Size on CT, Not on PET Images
- Abnormality Seen Only on First PET Image
- Assess the Patient’s Main Pathology Last
- Beware the Ureter
3. Excellent Views: The MIP, Coronal & Sagittal Images
- 3-D Rotating MIP & Coronal “Quick MIP”
- Coronal PET
- Sagittal PET
4. Written Annotations While Reading
- Numbers, Numbers & More Numbers
- Size & SUV Annotation System
- Sample Annotation Sheet
- Goals of Reporting
- Lawyers, Lawyers & Lawyers
- Sample PET/CT Report
- Negative Exam
- Positive Exam
- Patient Questionnaire
- Technologist’s Data Sheet
- Huge Exam: Requires Systematic Approach
- Our “12-Step Reading System”
- “The Read” in Action: Sample Case (Video)
- Annotations for Sample Case
- Final Report for Sample Case
Chapter 5: Normal Physiologic Distribution of FDG
"The essentials"
- To Locate Cancer, First Eliminate:
- Normal FDG-Avid “Structures”
- Benign FDG-Avid “Findings”
Chapter 6: Benign FDG-Avid "Findings" & Common Diagnostic Challenges
"Separating the Expert from the Not-So-Expert"
3. Chest
- Inflammatory Lymph Nodes
- Thymic Rebound
- Pleura: Talc Pleurodesis vs. Malignancy vs. Inflammation
-
Radiation-Induced Lung Disease
- Radiation Pneumonitis
- Radiation Fibrosis
- "Post-Therapeutic Inflammatory Changes" / Scarring of the Lung
- Atelectasis / Infiltrate
- Lipomatous Hypertrophy of the Inter-Atrial Septum
- Elastofibroma Dorsi
- Site of Prior Chest Port
- Esophagitis vs. Neoplasm
- Subcutaneous & Intramuscular Medical Injections
- Injected FDG-Blood Clot
4. Abdomen & Pelvis
- The Heterogeneous Liver
- Liver Ablation
- Hypermetabolic Geographic Fatty Infiltration
- Hypermetabolic Hepatic Adenoma
- FDG-Avid Adrenal Gland Algorithm
- Therapy-Induced Splenic Activation
- Peritoneal Carcinomatosis
- Pre-Sacral Soft Tissue After Rectal Surgery
- Gallbladder: Cholecystitis vs. Malignancy
- Inguinal Herniorraphy
- Bladder in Inguinal Canal
- Uterine Fibroid
- Tampon
5. Miscellaneous (continued)
-
Vascular Uptake
- Atherosclerosis
- Vasculitis
- Vascular Grafts
-
Value of NAC PET Images
- Resolving AC Artifacts
- Lung Nodule Identification
-
Non-Malignant, Yet Clinically Significant, FDG-Avid CT Abnormalies
- Acute Diverticulitis
- Colitis
- Cholecystitis
- Pneumonia
- Abscess
- Pancreatitis
- Skeletal Abnormalities [See Chapter 7]
Chapter 7: The Bones
"...is connected to the..."
Chapter 8: The Cancers
"Putting it all together"
Images Generated in a PET/CT Exam
Images Generated in a PET/CT Exam
Like most things in life, there is both good news and bad news regarding PET/CT scans.
The Good News: It’s a large exam. With only one exam, a patient’s entire body can be reliably evaluated for cancer.
The Bad News: It’s a large exam. There are many thousands of images generated, any one of which might contain the patient’s solitary focus of cancer.
CT Images:
CT images are obtained in the axial plane, with coronal and sagittal reconstructions. A typical study consists of anywhere from 750 axial images for a “skull base to mid-thigh” exam to 1500 images for a “whole body” study.
Non-Attenuation Corrected (NAC) Images:
These images are of limited diagnostic value. They are characterized by increased peripheral uptake along the skin of the patient, increased lung activity and relative decreased radiotracer uptake more centrally in the body.
Attenuation Correction (AC) Images:
In modern scanners, the CT images generated not only serve as the anatomic portion of the exam, but are also utilized for “attenuation correction” of the PET images, generating the much more useful AC PET images used for interpretation.
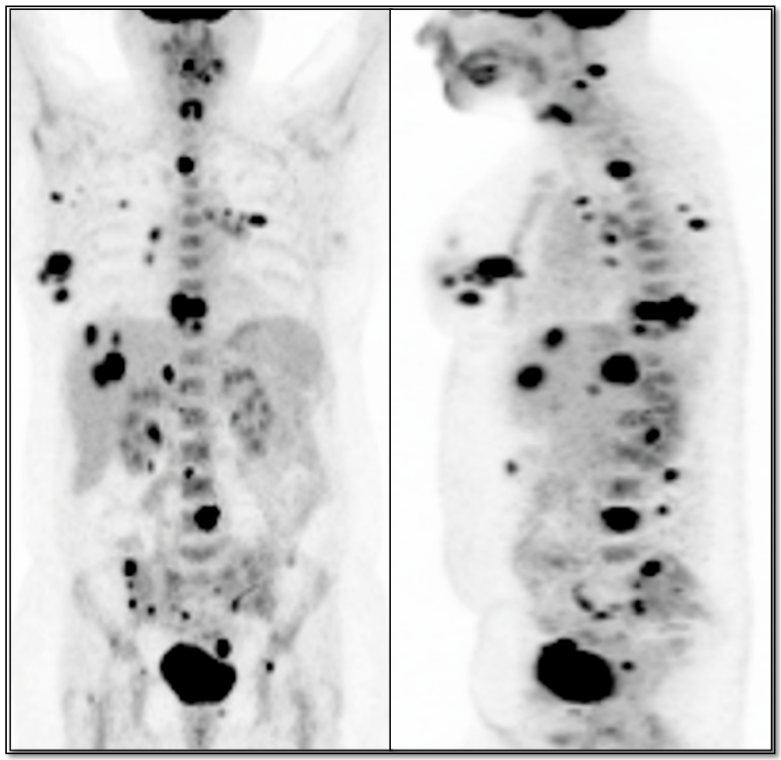
Maximum Intensity Projection (MIP Image):
Whole body MIP images can be viewed in rotation or static mode and provide an excellent overall assessment of disease (few radiologists are willing to confess the fact that more than 95% of their reported findings can be made from just the coronal MIP image!).
Fused CT & PET Images:
The CT images are fused with the AC PET images in the axial, coronal and sagittal planes – and evaluated using soft tissue, bone and lung window settings.
Final Images To Routinely Interpret:
- CT Images, soft tissue windows (3 planes) = 3 series
- CT Images, bone windows (3 planes) = 3 series
- CT Images, lung windows (axial plane) = 1 series
- Fused CT (soft tissue windows) & AC PET Images (3 planes) = 3 series
- Fused CT (bone windows) & AC PET Images (3 planes) = 3 series
- Fused CT (lung windows) & AC PET Images (axial plane) = 1 series
- AC PET Images, axial brain windows = 1 series
- NAC PET images (axial plane is usually sufficient) = 1 series
- MIP’s (static & rotating)
Therefore, a routine PET/CT exam results in 15 complete sets of images (most of which may be from the top of the head to the bottom of the feet) — clearly an extremely large exam consisting of many thousands of images.
Reading and interpreting a PET/CT exam, therefore, requires time, patience and an extremely organized reading scheme.
")